For decades, injectable testosterone has remained the backbone of testosterone replacement therapy (TRT). While transdermal and oral formulations have gained popularity, most American urologists and endocrinologists still rely on injectable esters for their predictable absorption and reliable outcomes. Yet, behind the apparent simplicity of an injection lies a nuanced clinical decision which ester to choose, at what interval, and for whom.
The three principal injectable esters used in the United States today testosterone enanthate, cypionate, and undecanoate share the same active hormone but differ in their chemical structure, half-life, and clinical handling. Choosing between them is not merely a matter of convenience or cost; it requires balancing pharmacokinetic properties, patient adherence, and individual physiology.
The central principle guiding this choice is one of equilibrium: the right ester must deliver stable testosterone levels without producing sharp peaks or deep troughs, while remaining practical and affordable for long-term use. In practice, this decision often reflects the urologist’s skill in integrating pharmacology with patient experience a blend of science and clinical art.
Overview of testosterone physiology, normal levels, and safe correction methods
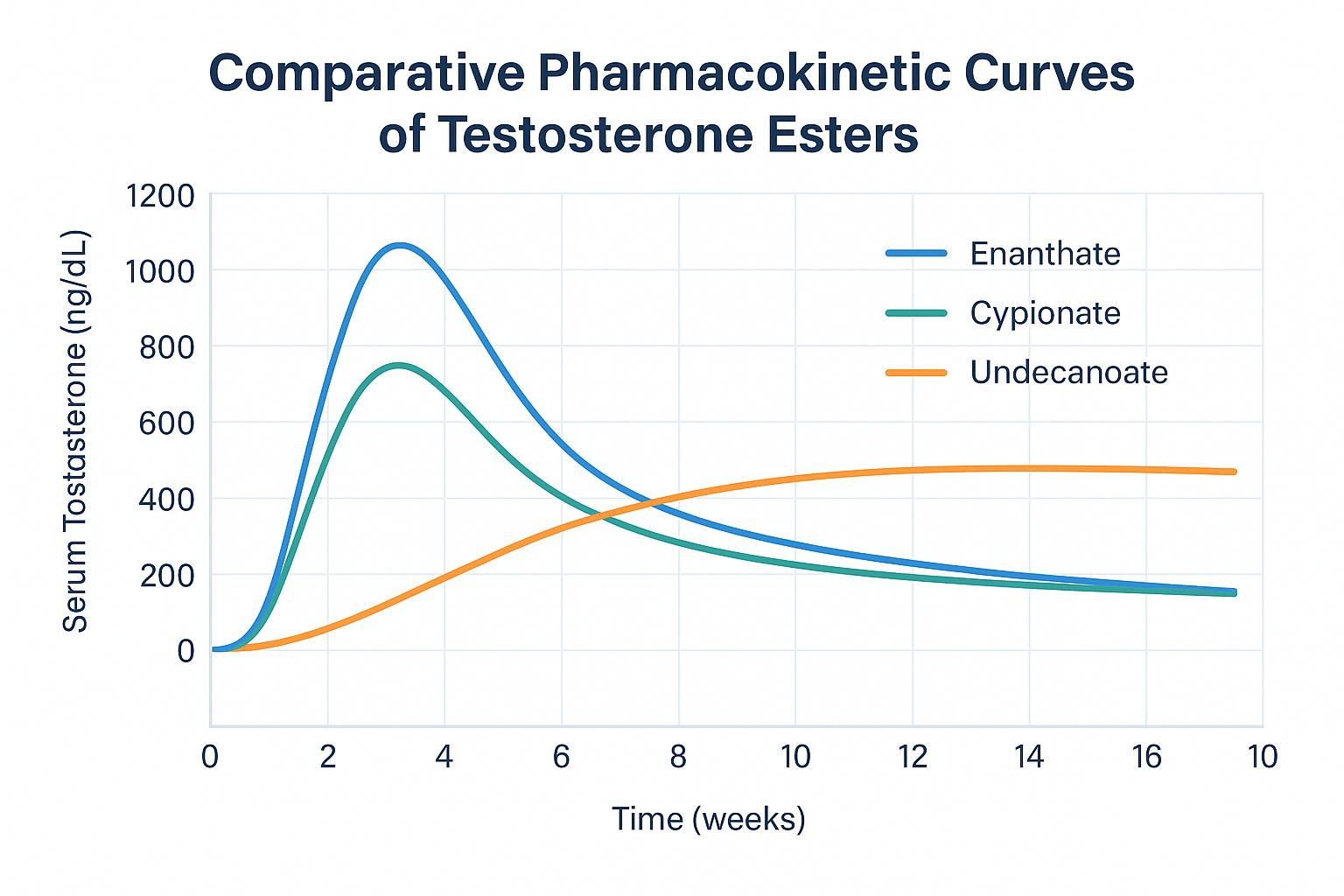
Each testosterone ester modifies the base molecule with a fatty acid chain that determines how slowly it is released from the injection site. The longer the ester chain, the slower the absorption and the longer the interval between injections. Understanding these kinetic profiles is essential, because the pattern of peaks and troughs directly affects how patients feel between doses. Testosterone enanthate and cypionate are the most widely used short – to medium-acting esters. Both provide effective hormone replacement, but their pharmacokinetics create different patient experiences. Enanthate typically reaches peak serum levels within 24–48 hours, followed by a gradual decline over the next 5–7 days. Cypionate behaves similarly but maintains a slightly longer plateau, often lasting up to 10 days due to subtle differences in its carbon chain and oil solubility. By contrast, testosterone undecanoate is a long-acting ester, with a half-life of approximately 10–12 weeks. It produces a remarkably smooth and sustained testosterone profile, minimizing the roller-coaster effect common with shorter esters. After the initial loading dose and a follow-up injection four weeks later, undecanoate maintains stable physiological concentrations with injections only every 10 to 12 weeks a dramatic difference in convenience. These pharmacokinetic distinctions have real clinical implications. Men using enanthate or cypionate may feel energized soon after injection, only to experience fatigue, irritability, or low libido as levels wane toward the end of the dosing cycle. In contrast, undecanoate users typically enjoy a flatter hormonal curve, but must attend clinic-based administrations because of its viscous formulation and risk of pulmonary microembolism if injected improperly. Another subtle yet meaningful difference lies in the carrier oil. Enanthate, often dissolved in sesame or cottonseed oil, releases slightly faster than cypionate, which is usually compounded in cottonseed or castor oil. This seemingly minor pharmacotechnical factor can shift absorption rate by several days enough to influence symptom stability in sensitive patients. In essence, shorter esters produce higher peaks and lower troughs, leading to noticeable hormonal fluctuations, while longer esters maintain smoother levels at the cost of flexibility and higher price. Illustration: serum testosterone concentration over time for enanthate (blue), cypionate (green), and undecanoate (orange). Shorter esters show sharp peaks and faster declines, while undecanoate maintains a steady plateau for several weeks. For many patients, injection frequency is the defining factor in treatment satisfaction. From a pharmacological standpoint, the choice between enanthate, cypionate, and undecanoate depends on how well a patient tolerates dosing intervals and how sensitive they are to fluctuations. In the United States, testosterone cypionate remains the most commonly prescribed injectable ester. Its pharmacokinetic profile allows for injections every one to two weeks, and its cost-effectiveness makes it accessible even without insurance coverage. Many clinicians prefer cypionate because it offers enough flexibility for individualized regimens weekly for stable levels, or biweekly for convenience. Enanthate, while nearly identical, tends to be favored in Europe and Canada, often given every seven to ten days. Some urologists choose enanthate for patients who are particularly sensitive to mood or libido swings, as its slightly faster clearance allows for tighter control of hormone peaks. Undecanoate (marketed as Aveed® in the U.S. and Nebido® in Europe) occupies a unique position. Its extended duration enables injections only once every 10 to 12 weeks after the initial titration phase. This long-acting formulation significantly improves adherence but comes with logistical trade-offs: it must be administered intramuscularly in a healthcare setting under observation, and its cost is higher than that of shorter esters. For men who prefer to avoid frequent injections or self-administration, however, undecanoate can provide unmatched stability. Convenience, therefore, is not the sole determinant it must be balanced with pharmacodynamics, accessibility, and clinical oversight. The urologist’s decision often depends on the patient’s comfort with self-injection, travel distance to clinic, financial factors, and personal rhythm of life. Ultimately, the best dosing schedule is the one that maintains steady-state testosterone levels within the mid-normal range (400–700 ng/dL), avoids abrupt hormonal swings, and fits the patient’s lifestyle and metabolic profile.
Pharmacokinetics and Serum “Peak–Plateau” Patterns
Injection Intervals and Dosing Convenience
Key parameters to monitor during testosterone treatment
Dose Titration and Trough Monitoring (“Timing Matters”)
Once a urologist selects the appropriate testosterone ester, the next challenge lies in maintaining the right serum concentration over time. Unlike most medications with straightforward dosing, testosterone therapy requires careful titration – not only to normalize laboratory numbers but to stabilize symptoms. The objective is simple in theory yet complex in practice: keep testosterone levels within the mid-physiological range (roughly 400–700 ng/dL) while avoiding peaks that cause irritability or troughs that trigger fatigue.
The term “trough level” refers to the lowest point in serum testosterone concentration before the next scheduled injection. Measuring testosterone at this point provides a reliable indicator of overall hormonal exposure and helps prevent both underdosing and overcorrection. For example, with short-acting esters like cypionate or enanthate, blood should typically be drawn the morning before the next injection. With undecanoate, due to its longer duration and flatter curve, timing is less critical, but a standardized sampling protocol such as just prior to the next 10–12-week injection ensures consistency.
Clinical titration relies on both biochemical and subjective feedback. Laboratory values confirm adequacy, but equally important are patient-reported metrics: libido, energy, mood, and cognitive clarity. Many clinicians adjust dosing intervals rather than total dose to fine-tune therapy for instance, shifting cypionate injections from biweekly to weekly if mood swings emerge near the end of each cycle.
An optimal titration strategy aims to eliminate “roller-coaster” fluctuations while respecting each patient’s metabolism, activity level, and lifestyle. Proper timing and open communication between patient and clinician are often what differentiate a successful therapy from a frustrating one.
Managing Mood and Libido Fluctuations
Hormonal balance has profound psychological implications. Men undergoing testosterone therapy frequently describe emotional variability that parallels the rise and fall of serum testosterone. Sudden spikes may produce transient euphoria or irritability, while declining levels can bring fatigue, loss of motivation, and diminished libido.
Shorter esters, such as enanthate and cypionate, are particularly prone to these effects due to their rhythmic peaks and troughs. For such patients, urologists often recommend dividing the dose into smaller, more frequent injections for instance, every seven days instead of every fourteen to achieve a smoother hormonal curve. This adjustment can significantly reduce mood volatility and maintain consistent sexual desire throughout the cycle.
In contrast, testosterone undecanoate, with its long half-life, provides a steadier emotional baseline. However, because of its extended dosing interval, any side effect (such as fluid retention or hematocrit rise) may persist longer before correction is possible. Thus, the clinician must balance psychological stability with the practicality and reversibility of each ester.
Beyond pharmacokinetics, lifestyle plays a crucial role. Sleep deprivation, alcohol use, stress, and sedentary behavior amplify mood swings independent of hormonal levels. Combining testosterone therapy with regular exercise, structured sleep, and mindfulness interventions can greatly enhance emotional equilibrium.
Modern practice embraces the principle of shared decision-making. Patients who understand the pharmacology of their treatment are more likely to adhere, report symptoms accurately, and participate actively in dosage adjustments turning therapy into a collaborative, safe, and personalized process.
Common Dosing Errors and How to Avoid Them
Despite clear guidelines, dosing mistakes remain common in testosterone replacement therapy. They typically fall into two categories: administration errors and interpretation errors.
One of the most frequent clinical pitfalls is overextending injection intervals with short esters. When enanthate or cypionate is administered every three or even four weeks a pattern still seen in general practice testosterone levels plummet long before the next dose, producing exaggerated hormonal oscillations. Patients often misinterpret the resulting fatigue as a need for higher doses, leading to an unnecessary cycle of escalation.
Another common error involves lab timing. Drawing blood too soon after injection (during the peak phase) yields falsely elevated testosterone readings, causing the clinician to reduce dosage incorrectly. Conversely, testing several days too late may exaggerate trough levels and prompt unwarranted dose increases. The consequence is biochemical instability that undermines patient confidence in therapy.
A subtler, but equally important, mistake occurs when milligrams per milliliter are confused with total dose volume. Given the variation in concentration among pharmaceutical and compounded products, urologists stress meticulous record-keeping and education for self-injecting patients.
Finally, ignoring hematocrit and PSA monitoring can turn a well-intended therapy into a risky endeavor. Elevated hematocrit (>54%) increases thrombotic risk, while neglected prostate screening may delay detection of pre-existing malignancy.
Ultimately, avoiding these errors depends on systematic follow-up, patient education, and adherence to evidence-based dosing intervals.
Comparative Overview of Testosterone Esters
To synthesize these distinctions, the following table outlines key pharmacologic and practical differences among the three principal injectable esters used in testosterone therapy.
| Ester | Half-life | Injection Interval | Common Brand (U.S.) | Advantages | Limitations |
|---|---|---|---|---|---|
| Enanthate | 4–5 days | Every 7–10 days | Delatestryl® | Flexible dosing, low cost | Peaks & troughs, frequent injections |
| Cypionate | 5–7 days | Every 7–14 days | Depo-Testosterone® | Widely available, steady levels | Same fluctuation risk as enanthate |
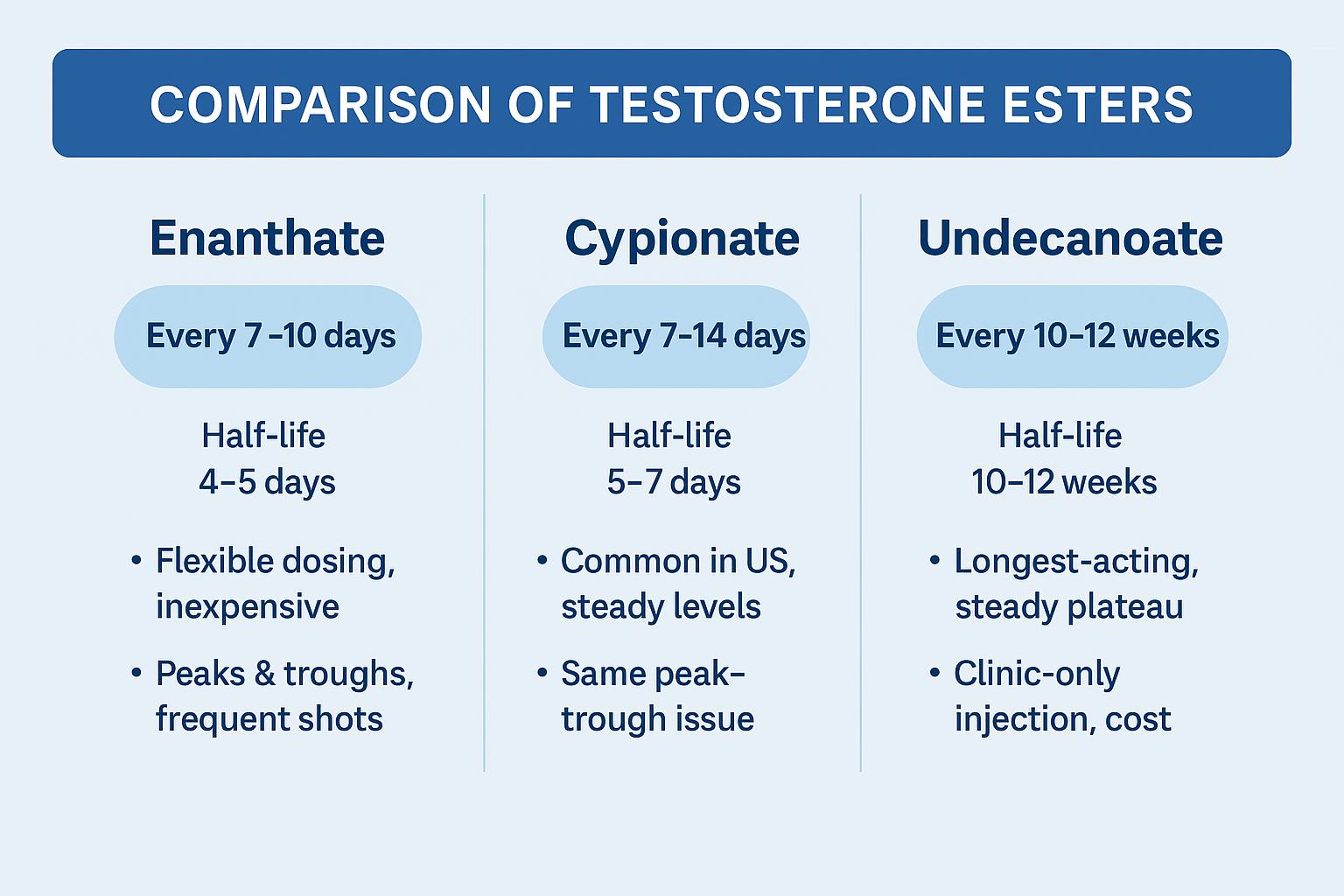
| Undecanoate | 10–12 weeks | Every 10–12 weeks | Aveed® (US) / Nebido® (EU) | Long-acting, stable plateau | Clinic-only administration, higher cost |
Visual summary of pharmacologic and practical differences among enanthate, cypionate, and undecanoate. Each column displays injection frequency, half-life, and characteristic advantages.
Proper interpretation of these data underscores that no single ester is superior for all patients. Enanthate and cypionate offer flexibility and affordability; undecanoate delivers unmatched stability but requires clinical oversight. For urologists, the decision is not about choosing the “best” compound but rather the right one for each patient’s physiology, routine, and goals.
Summary and Key Takeaways
The selection of a testosterone ester whether enanthate, cypionate, or undecanoate reflects far more than a matter of convenience or availability. It represents a deliberate clinical choice grounded in pharmacology, patient physiology, and individualized goals.
Shorter esters like enanthate and cypionate provide flexibility and are ideal for men who can self-inject regularly or require dose adjustments based on symptoms. They allow tighter control of hormone levels but demand discipline and frequent monitoring. In contrast, long-acting testosterone undecanoate offers unparalleled stability and convenience, though at the cost of reduced flexibility, higher price, and the need for clinic-based administration.
From a urologist’s perspective, the decision-making process integrates three parallel dimensions:
- pharmacokinetic behavior and serum stability,
- patient adherence and tolerance to injection intervals,
- safety and long-term monitoring of hematocrit, PSA, and cardiovascular health.
Clinical outcomes improve dramatically when therapy is personalized when injection intervals are titrated to symptoms and trough levels, and when patients are educated to recognize the subtle differences between underreplacement and excess. The best TRT regimen, therefore, is not the strongest or longest-acting one, but the most stable, safe, and sustainable for each individual.
Frequently Asked Questions (FAQ)
When should I choose testosterone undecanoate instead of enanthate or cypionate?
Long-acting testosterone undecanoate suits men who prefer fewer injections and stable levels. Shorter esters like enanthate or cypionate are better when frequent dose adjustments or self-administration are needed.
Does the type of ester affect how often I need injections?
Yes. Enanthate and cypionate are typically injected every 7–14 days, while undecanoate lasts 10–12 weeks between doses.
How important is blood-draw timing for monitoring TRT?
Timing is crucial. Testosterone should be checked at the trough (just before the next dose) to prevent under- or overdosing.
What mistakes are most common in testosterone therapy?
Over-stretching injection intervals and testing blood at the wrong time are frequent errors. Ignoring hematocrit or PSA monitoring can also compromise safety.
How can I know which testosterone ester fits me best?
The choice depends on your lifestyle, budget, and clinical goals. Your urologist will balance pharmacokinetics, convenience, and safety to personalize therapy.
References
- American Urological Association (AUA) – Testosterone Deficiency Guideline (2024)
- The Endocrine Society – Testosterone Therapy in Men with Hypogonadism: Clinical Practice Guideline (2024 Update)
- U.S. Food and Drug Administration (FDA) – Class-wide Labeling Changes for Testosterone Products (Feb 28, 2025)
- JAMA Cardiology – FDA Updates Testosterone Labeling for Blood Pressure Monitoring (2025)
- The Androgen Society – Press Release on FDA Changes (March 2025)